
The Systemic Pathology of Policy Fatigue: An Exhaustive Analysis of Compliance Failure, False Declarations, and Frontline Risk
1. Introduction: The Paradox of Governance
In the contemporary organizational landscape, the volume of regulation intended to mitigate risk has paradoxically generated a secondary, systemic risk: policy fatigue. This phenomenon, characterized by the reduced capacity or willingness of individuals to formulate, absorb, or adhere to regulations following periods of intensive legislative activity or information overload, represents a critical deceleration of adaptive governance. As organizations attempt to insulate themselves from liability through comprehensive policy frameworks, they inadvertently create an environment of cognitive saturation. In this environment, the primary mechanism of compliance shifts from genuine comprehension to performative adherence, manifested behaviorally through "false declarations"—the signing of acknowledgments without reading—and "skim-reading," where critical safety or compliance details are cognitively filtered out.
The genesis of this report lies in the observation that "tick-box" compliance cultures do not merely fail to prevent accidents; they actively incubate them. From the catastrophic failure of the Piper Alpha oil platform to the systemic ethical collapse at Wells Fargo, the historical record suggests that when the cognitive load of compliance exceeds human capacity, "rational withdrawal" occurs. This withdrawal leads to a collapse in frontline performance, where the "paper program" of safety diverges sharply from the operational reality.
This report provides an exhaustive examination of policy fatigue. It moves beyond anecdotal observation to scrutinize the psychological mechanisms, legal implications, and operational catastrophes driven by this phenomenon. Drawing on an extensive review of data from the aviation, healthcare, financial, and energy sectors, the analysis dissects the anatomy of "signing without reading," the erosion of the "duty to read" doctrine in the face of incomprehensible "legalese," and the rising standard of "effectiveness" demanded by regulators like the Department of Justice (DOJ). Furthermore, it evaluates the efficacy of modern mitigation strategies, positing that the only viable solution is a fundamental restructuring of how governance is designed and delivered.
2. The Anatomy of Policy Fatigue: Phenomenology and Mechanism
To effectively address the issue of policy fatigue, it is necessary to establish a precise nomenclature and theoretical framework. The term "fatigue" in this context moves beyond simple physiological tiredness; it describes a specific degradation in the executive function of decision-making and adherence caused by the relentless accumulation of mandates.
2.1 Defining the Construct
The Sustainability Directory formally defines Policy Fatigue as "the state of reduced capacity or willingness among governments, organizations, or the public to formulate, absorb, or adhere to new regulations, guidelines, or mandates, often following a period of intensive or rapidly changing legislative activity". Etymologically derived from the Greek politeia (citizenship/government) and Latin fatigare (to exhaust), the term captures a diminished responsiveness to regulatory changes after prolonged exposure to numerous, complex, or contradictory mandates.
While the term has gained traction in public health contexts—specifically "Pandemic Fatigue," defined as a broad decline over time in support and adherence across mitigation behaviors —its application in corporate governance is equally profound. In the corporate sphere, this translates to Compliance Fatigue, where a saturation of rules leads to disengagement, skepticism, and a "tick-box" mentality. The literature suggests that as behavioral mitigation measures or corporate policies continue to accumulate, fatigue is reflected in a monotonic decrease in support and adherence that cannot be explained by other causes.
This phenomenon is distinct from, yet intimately related to, other forms of cognitive exhaustion:
Table 1: Taxonomy of Fatigue Constructs in Compliance Contexts
| Construct | Definition | Relationship to Policy Fatigue | Sources |
| Decision Fatigue | A deterioration in the quality of choices made after a long session of decision-making. | Pertains to the depletion of the brain's finite capacity for rational choice. Policy fatigue exacerbates this by forcing constant micro-decisions regarding compliance. | |
| Alert Fatigue | Desensitization to safety alarms or notifications due to high frequency and low positive predictive value. | A specific subset of policy fatigue where "rational withdrawal" of attention occurs; critical warnings are ignored alongside trivial ones. | |
| Text Blindness | A state where, despite visual acuity, an individual loses the power to interpret written language due to cognitive overwhelm. | Represents the extreme physiological endpoint of reading long policies; the "power of sight" remains but the "power of interpretation" fails. | |
| Green Fatigue | Burnout from constantly attempting to make environmentally perfect choices. | Parallels policy fatigue in the sustainability sector; consumers abandon ethical criteria due to the impossibility of processing all certification labels. |
2.2 Cognitive Load Theory and the Limits of Processing
The primary driver of policy fatigue is Cognitive Load. Academic analysis suggests that high cognitive effort depletes glucose, causing a sensation of central fatigue that mimics physical tiredness and reduces the motivation to be active. In the context of reading policies, Cognitive Load Theory (CLT) posits that the human working memory has a limited capacity. When policies are drafted in dense "legalese" or distributed in massive volumes, they impose an "extraneous cognitive load"—mental effort that does not contribute to learning but is wasted on deciphering poor presentation.
This overload triggers a "systemic deceleration of adaptive governance". When the brain is overwhelmed by the volume of information (e.g., hundreds of pages of employee handbooks), it defaults to heuristic processing. Rather than engaging in the deep semantic processing required for true comprehension, the brain utilizes shortcuts: skimming, scanning for keywords, or simply signing the declaration to remove the stimulus. This is not merely a failure of will; it is a physiological protective mechanism against cognitive depletion.
Research into "notification fatigue" further illuminates this mechanism. Continuous "pings" or policy updates create a cycle of micro-decisions that deplete cognitive energy. Every time a new policy is released, the brain must evaluate its urgency and relevance. This continuous process creates a drain on cognitive resources, leaving mental energy unavailable for the actual substantive work the employee is hired to perform.
2.3 Policy Cynicism and "The Flavor of the Month"
When frontline workers are subjected to continuous, inconsistent, or rapidly changing policies, they experience Policy Cynicism. This is a defensive psychological posture where new policies are viewed not as genuine operational improvements, but as "the political flavor of the month".
Studies indicate that policy cynicism acts as a formidable barrier to implementation. If frontline workers perceive that policies do not guarantee an acceptable level of autonomy, or if the policies appear disconnected from operational reality, support for the program collapses. This creates a "rational withdrawal" from engagement. Workers do not necessarily disagree with the abstract goals of safety or ethics; they disagree with the specific bureaucratic manifestation of those goals (the policy), viewing it as an impediment to their actual work.
The danger of policy cynicism is that it leads to "compliance fatigue," where the social traction of a rule fades, preventing policy fatigue or reversal only if the "cultural coefficients" of the organization are strong. If governments or corporations repeatedly introduce and then abandon initiatives, the workforce develops a "Bend over, here it comes again" attitude, leading to superficial compliance. This cynicism is the precursor to the "tick-box" culture, where the appearance of compliance is prioritized over the substance of risk management.
3. The Psychology of False Declarations: "Signing Without Reading"
One of the most pervasive and dangerous manifestations of policy fatigue is the act of signing a compliance declaration without reading the underlying text. This behavior, often termed "signing without reading" or "clicking without reading," is not an aberration; it is a statistical norm driven by structural, linguistic, and psychological factors.
3.1 Prevalence and Demographics of Non-Reading
The behavior of signing unread documents is ubiquitous and transcends demographic boundaries. Research indicates that signing without reading is common across the board, from consumers to highly trained professionals. In larger organizations, statistics are alarming: approximately 61% of employees admit to signing employment contracts or policies they did not fully understand.
Crucially, this behavior appears resistant to negative feedback, suggesting deeply ingrained psychological drivers. Surveys show that even among individuals who previously lost money or faced negative consequences due to unread terms, 61% admitted they still do not thoroughly read contracts afterwards. This illustrates that the behavior is not merely a result of ignorance, but of a calculated (consciously or subconsciously) trade-off between time and risk.
In the digital realm, this phenomenon is exacerbated. Users tend to weigh the benefits of joining a network or completing a task against the cost of reading terms. When "friends" are already in the network, or when the job requires the software, agreeing to terms becomes "irrelevant or insignificant". The act of clicking "I Agree" is stripped of its contractual significance and reduced to a mechanical gateway interaction.
3.2 The "Empire of Forms" and Rational Withdrawal
Scholars describe the overwhelming prevalence of standard form contracts as the "Empire of Forms," where terms are so embedded and non-negotiable that reading them becomes a futile exercise. This environment fosters Rational Withdrawal.
In economic game theory, rational withdrawal occurs when the marginal returns of an activity (reading a policy) diminish to the point where they are outweighed by the cost (time/effort). If an employee believes they have no power to negotiate the terms of a cybersecurity policy, and the policy is 40 pages long, the "rational" strategy is to sign immediately to return to productive work. The probability of finding a "deal-breaker" clause is perceived as low, while the cost of reading is immediate and high.
This rational withdrawal is distinct from laziness; it is an economic decision regarding the allocation of attention. In the context of "HiAP (Health in All Policies) fatigue," for example, burnout develops from continuous, resource-intensive assessment processes that fail to produce demonstrable results. Similarly, in corporate compliance, if employees feel that reading the policy will not change their ability to influence it, they withdraw their attention.
3.3 The Linguistic Barrier: "Legalese" and Comprehension
The complexity of policy language is a deliberate and significant barrier to comprehension. Legal documents and corporate policies are infamous for dense "legalese" that the average person—and even the average lawyer—finds impenetrable.
Table 2: The Impact of Legal Register on Comprehension
| Factor | Findings | Source |
| Recall Accuracy | Lawyers and laypeople alike show significantly lower recall for content drafted in "legalese" compared to simplified registers. | |
| Preference | Transactional lawyers and judges prefer plain English over traditional legal phrasing. | |
| Enforceability Perception | Lawyers rate simplified contracts as equally enforceable to legalese contracts, debunking the myth that complexity is required for legal weight. | |
| Hypothesis | The persistence of legalese is attributed to the "curse of knowledge" (lawyers do not realize how complex they sound) and tradition, rather than necessity. |
This linguistic complexity contributes directly to policy fatigue. When an employee opens a Code of Conduct and encounters archaic phrasing, the "extraneous cognitive load" spikes, leading to immediate disengagement. The document signals that it is written for legal defense, not for employee guidance. This "text blindness"—where the visual ability to read exists but the intellectual ability to decode is thwarted by complexity—renders the policy functionally invisible.
Furthermore, the "tick-box" nature of compliance creates a "compliance fatigue" where the social traction of the policy fades. The employee signs the document not as an act of assent, but as an act of submission to a bureaucratic requirement that appears divorced from their actual duties.
4. The Legal Landscape: Enforceability of Unread Policies
The disjunction between the psychological reality of policy fatigue and the legal presumption of the "duty to read" creates significant corporate risk. While employees often sign without reading, the legal system is increasingly scrutinizing the validity of such assent, particularly when "constructive knowledge" is claimed in the face of demonstrable obfuscation.
4.1 The "Duty to Read" Doctrine vs. Modern Reality
Historically, contract law has relied on the "duty to read" doctrine, which holds that a party is bound by the provisions in an agreement they sign, even if they have not read them. The rationale is that courts do not wish to reward negligence. A party who signs without reading is presumed to have accepted the risk of the unknown terms.
However, this doctrine is eroding. Courts are increasingly acknowledging the reality of "signing without reading" in the context of Adhesion Contracts—standard forms offered on a "take it or leave it" basis. This is particularly relevant in employment contexts where there is a gross disparity in bargaining power. When a policy is extremely long and the employer knows that "policy fatigue" prevents reading, relying on the "duty to read" may no longer be a guaranteed defense.
4.2 Unconscionability and the "Sliding Scale"
To address the inequity of enforcing unread standard terms, courts employ the doctrine of Unconscionability. This doctrine typically requires a showing of both procedural and substantive unconscionability :
- Procedural Unconscionability: Arises from "surprise" (undisclosed terms buried in fine print) and "oppression" (lack of negotiation power). Long, complex policies that are signed under time pressure—a symptom and driver of policy fatigue—may be deemed procedurally unconscionable.
- Substantive Unconscionability: Refers to terms that are overly harsh or one-sided.
California courts, for example, use a "sliding scale" approach: the more procedurally unconscionable the contract (e.g., a dense, 50-page employee handbook forced on a low-wage worker), the less substantive unconscionability is required to invalidate it. If policy fatigue is induced by the employer's design (intentional length and complexity), courts may refuse to enforce buried terms like arbitration clauses.
4.3 Constructive Knowledge and "Click-Through" Risks
Employers often rely on Constructive Knowledge—the idea that because an employee could have read the policy, they are presumed to know its contents. However, the digital mechanism of delivery matters significantly.
Research into online agreements distinguishes between "clickwrap" (where a user must actively click "I Agree") and "browsewrap" (where terms are merely posted via a link). While clickwrap agreements are generally enforceable (70% success rate in one study), browsewrap agreements are enforceable only 14% of the time. This suggests that "manifest assent" requires an active interaction.
However, even clickwrap is under threat if the interaction is perfunctory. If an employee clicks "I Agree" in 2 seconds on a document that takes 30 minutes to read, the assent is "rational withdrawal" in action. The danger for corporations lies in the "Paper Program" defense. If an employee violates a policy (e.g., insider trading or safety violation), and the company's only defense is a "click-through" receipt from a 50-page PDF that was opened for mere seconds, regulators (like the DOJ) may view the compliance program as ineffective.
4.4 The DOJ's Shift to "Effectiveness"
The U.S. Department of Justice (DOJ) has fundamentally shifted its evaluation criteria for corporate compliance programs. It no longer asks merely "Does the company have a policy?" but rather "Is the program effective in practice?".
Table 3: DOJ Evaluation Criteria Relevant to Policy Fatigue
| Criteria | Key Question for Regulators | Implication for Policy Fatigue |
| Accessibility | Are policies published in a searchable format? Can employees find them? |
Policies buried in static PDFs induce fatigue; searchable, accessible tools reduce it. |
| Design | Is the training "check-the-box" or tailored to risk? |
Generic, long training modules are viewed as ineffective. Training must be relevant to the role to avoid fatigue. |
| Engagement | Does the company track how employees engage with policies? |
Mere click-throughs are insufficient. Regulators look for evidence of understanding and "speak up" culture. |
| Resourcing | Is the program adequately resourced? |
Under-resourced teams cannot update policies frequently enough to keep them relevant, leading to stale, ignored rules that induce cynicism. |
The DOJ explicitly states that a "paper program"—one that exists only in manuals but is not integrated into daily work—is a sign of an ineffective compliance culture. Consequently, relying on false declarations (signatures without reading) exposes the corporation to heightened liability in the event of an investigation.
5. The "Tick-Box" Culture: Impact on Frontline Quality and Safety
When policy fatigue sets in, compliance transforms from a mindset of active risk management to a bureaucratic ritual known as "Tick-Box Culture." This shift is not benign; it is a known precursor to industrial disasters and healthcare failures. It represents the "displacement" of safety by the administration of safety.
5.1 The Mechanism of Failure: Procedure Complexity and Habituation
In safety-critical industries (aviation, oil & gas, healthcare), procedures are designed to prevent error. However, as Procedure Complexity increases, the likelihood of human error rises. Studies in maritime operations show that "procedure" and "fatigue" are primary factors affecting error probability, with complex tasks having significantly higher error rates.
The relationship is non-linear. As procedures become more prescriptive and detailed to cover every liability, they become less usable. This leads to Habituation:
- Warning Habituation: Repeated exposure to the same visual or written warnings leads to a decrease in response. Workers stop "seeing" the warning, similar to how one ignores a ticking clock or background noise.
- Dishabituation Failure: Even when hazards change, if the warning format remains static (e.g., standard boilerplate safety text), workers fail to re-engage attention.
- The "Cry Wolf" Effect: If policies are constantly changed or alerts are triggered for minor issues (Alert Fatigue), workers develop a "rational withdrawal" of attention, ignoring critical warnings alongside trivial ones.
5.2 Case Study: The Piper Alpha Disaster
The 1988 Piper Alpha oil platform explosion, which killed 167 men, stands as the definitive case study of policy fatigue and tick-box culture. The Cullen Inquiry revealed that the platform had a "Permit to Work" system—a strict policy for managing hazardous tasks. However, the investigation found fundamental failures rooted in policy fatigue:
- The System was a Paperwork Exercise: The task of drawing up safety cases became "essentially a paperwork and 'tick-box' exercise" rather than a living risk assessment. The focus was on completing the form, not assessing the risk.
- Procedure Fatigue: The sheer volume of procedures meant that they were followed in form but not in spirit. The inquiry noted that a "tick box approach and detailed prescriptive regulation" failed to instill a culture of safety.
- Operational Disconnect: A safety valve was removed for maintenance, but the paperwork did not effectively communicate this status across shifts due to the bureaucratic noise. The isolation procedure was technically "ticked," but the communication failed.
This disaster underscores that prescriptive regulation can induce policy fatigue, where the focus shifts to "compliance with standards" rather than "understanding of risks".
5.3 Case Study: Healthcare and the Mid Staffordshire Scandal
In the healthcare sector, policy fatigue manifests as a prioritization of administrative targets over patient care. The Francis Report on the Mid Staffordshire NHS Foundation Trust scandal identified a "tick-box culture" as a primary cause of appalling neglect.
- The Phenomenon: Nurses were overwhelmed by "an industry of paperwork" created to provide assurance of care. This bureaucratic load displaced the actual delivery of care.
- Compassion Fatigue via Policy: The pressure to meet metrics (e.g., waiting time targets) meant that staff "treated patients in the manner described" (neglectful, rude) because the system prioritized the record of the learning episode or care event over the event itself.
- Outcome: Patients were left in soiled bedding or without water because staff were focused on complying with the administrative superstructure. The policy "fatigue" here was literal: staff were exhausted by the demands of the system and had no capacity left for empathy or observation.
Research into Intentional Rounding—a policy introduced to fix these issues—found that it too became a "tick-box" exercise. Nurses would complete the rounding documentation without engaging meaningfully with the patient, proving that adding more policy to cure policy fatigue is a failed strategy.
6. Corporate Governance Failures: The High Cost of Ineffective Compliance
In the financial and corporate sectors, policy fatigue leads to massive regulatory penalties and reputational ruin. The Department of Justice (DOJ) and financial regulators have moved away from accepting the mere existence of policies as a defense, now focusing on whether policies are understood, internalized, and followed.
6.1 Wells Fargo: The Failure of "Paper Programs"
The Wells Fargo cross-selling scandal is a paradigm of policy fatigue and cultural dissonance. It illustrates what happens when written policies conflict with operational incentives.
- The Policy vs. The Reality: Wells Fargo had Codes of Conduct and policies prohibiting the creation of fake accounts. However, the pressure to meet sales quotas ("Eight is Great") was the dominant signal. Employees experienced "policy cynicism," viewing the ethical code as "the political flavor of the month" while the sales targets were the reality.
- The Compliance Failure: The Office of the Comptroller of the Currency (OCC) and the Consumer Financial Protection Bureau (CFPB) found material deficiencies in the bank's compliance risk management and training. The "training" was ineffective because it was likely treated as a tick-box exercise by employees who were simultaneously being "hounded, berated, and demeaned" to break the rules.
- Consequence: The bank faced billions in fines and consent orders requiring total overhauls of risk management. The consent orders specifically cited the failure to "develop and implement compliance training" that was effective, highlighting that the mere existence of training modules is insufficient if the culture negates them.
6.2 Citigroup: Data Quality and Consent Orders
Similarly, Citigroup has faced repeated consent orders related to data quality and compliance risk management.
- The Issue: Ongoing deficiencies in data quality management and internal controls. When data governance policies are complex and data entry is burdensome, employees experience fatigue, leading to poor data quality.
- The Consequence: A $400 million civil money penalty and a requirement to overhaul the entire risk and control environment.
- The Lesson: "Policy fatigue" in data entry (the "tick-box" of entering data just to get it done) undermines the foundational data required for risk management. If employees are fatigued by the process, the data they produce is garbage, rendering the sophisticated risk models built on top of it useless.
6.3 Morgan Stanley: The Protective Value of Avoiding Fatigue
Conversely, Morgan Stanley's handling of the Garth Peterson FCPA (Foreign Corrupt Practices Act) case demonstrates the protective value of a compliance program that actively combats policy fatigue.
- The Incident: Peterson, a managing director, circumvented internal controls to bribe Chinese officials.
- The Defense: Morgan Stanley demonstrated that it had not just "issued" a policy, but had trained Peterson specifically on the FCPA seven times and sent 35 compliance reminders. Peterson had also signed multiple annual certifications.
- The Outcome: The DOJ and SEC issued a "declination"—they charged Peterson individually but did not prosecute Morgan Stanley.
- Insight: The frequency and targeted nature of the training—preventing the "one-and-done" fatigue—allowed the company to prove that Peterson's actions were those of a rogue employee, not a systemic failure. The program was not a "paper program" but a living, breathing control system.
7. Metrics, Mitigation, and Modernization
To combat policy fatigue, organizations must first detect it and then deploy strategies that align with human cognitive limits. Traditional metrics (e.g., "100% completion rate") are often misleading indicators of "click-through compliance."
7.1 Measuring the Unmeasurable: Beyond Completion Rates
High completion rates for policy acknowledgments often mask deep policy fatigue. If an employee completes a 30-minute module in 3 minutes, they have not complied; they have "gamed" the system. Organizations must move toward "outcome-based" measurement.
Table 4: Metrics for Detecting Policy Fatigue
| Metric | Indication | Source |
| Time-Spent Analysis | Tracking "average time spent per course" flags rushed learners. Consistent speeding indicates disengagement. | |
| Readership Rates | Tracking unique opens and dwell time on policy documents creates a "heat map" of compliance. Low rates suggest "banner blindness." | |
| Quiz Accuracy | Low scores on first attempts, followed by rapid retries, indicate skimming and guessing rather than learning. | |
| Help Desk Queries | A lack of questions about a complex new policy might indicate no one read it. A spike in questions indicates engagement. | |
| Shadow IT Usage | The use of unapproved tools is a behavioral signal that the official policy is too restrictive or complex ("procedure fatigue"). |
7.2 Rational Withdrawal of Policies ("Deprescribing")
Just as physicians practice "rational withdrawal" of medications to reduce polypharmacy side effects in the elderly, organizations must practice Rational Withdrawal of Policies.
- Concept: Discontinuing or simplifying low-value policies to preserve cognitive capacity for high-risk rules.
- Mechanism: Reducing the volume of rules reduces the "noise," allowing the "signal" of critical safety rules to be heard. This mitigates "Compliance Fatigue" where the sheer number of mandates creates resistance.
- Application: In "HiAP fatigue" (Health in All Policies), streamlining assessments for small policies ensures resources are concentrated on high-impact projects. The same logic applies to corporate policies: sunset clauses and periodic reviews are essential to prevent accumulation.
7.3 Microlearning and "Just-in-Time" Training
Microlearning involves delivering content in small, focused bursts (3–5 minutes) rather than hour-long sessions. This strategy directly addresses Cognitive Load Theory.
- Retention: Research indicates microlearning improves knowledge retention by 50% compared to traditional methods and improves completion rates from 20-30% to 83%.
- Efficiency: Development costs are lower, and speed of deployment is faster (300% faster), allowing training to stay relevant to current risks.
- Mechanism: "Just-in-time" delivery ensures the policy is read when it is needed (e.g., reading the gift policy right before the holiday season), increasing relevance and decreasing the "extraneous cognitive load" of processing irrelevant information.
7.4 Gamification: Combating Boredom and Cynicism
Gamification applies game-design elements (leaderboards, badges, interactive scenarios) to non-game contexts to combat the boredom associated with compliance.
- Statistics: Gamified training can increase engagement by up to 48% and motivation by 90%.
- Psychology: It counters "policy cynicism" by providing instant feedback and a sense of progress. Employees retain 22% more information when trained using gamified solutions.
- Caveat: It must be substantive. Superficial gamification can be perceived as trivializing serious risks, potentially increasing cynicism if not executed well.
7.5 Designing for Usability: The "Plain Language" Imperative
The "usability of procedures" is a safety-critical factor. Policies must be designed for the user, not the lawyer.
- Visual Aids: Using infographics and flowcharts reduces the "text blindness" associated with walls of text. Visualization dashboards reduce the time spent collecting data and the cognitive load.
- Legal Validity: As noted, simplified contracts are rated as preferable and equally enforceable by legal experts. The argument that "we need legalese for protection" is factually incorrect and operationally dangerous.
- Testing: Procedures should be "road-tested" for usability. If a worker cannot perform the task while following the procedure, the procedure is defective.
8. Conclusion: From Fatigue to Fluency
Policy fatigue is not merely an administrative nuisance; it is a systemic pathology that corrodes the protective layer of governance. The evidence from Piper Alpha, Mid Staffordshire, and Wells Fargo converges on a single truth: when the demand for compliance exceeds the cognitive capacity of the workforce, the result is not safer operations, but a "tick-box" illusion of safety that masks accumulating risk.
The behavior of "signing without reading" is a rational adaptive response to an irrational environment of "legalese" and information overload. While the legal system currently upholds the "duty to read" in many jurisdictions, the shifting landscape of unconscionability and the DOJ's focus on "effectiveness" suggests that the era of the "Paper Program" is ending. Corporations can no longer hide behind signed receipts for unread policies.
To restore integrity to the frontline, organizations must treat attention as a finite resource. This requires the "rational withdrawal" of obsolete rules, the adoption of microlearning to match cognitive bandwidth, and the rigorous simplification of language. Only by making the "safe choice the easy choice" and reducing the cognitive burden of compliance can organizations move beyond the fatigue of regulation to the reality of commitment. The cost of failing to do so is not just measured in fines, but in lives and livelihoods lost to the entropy of the "Empire of Forms."
Why the Professional Standards Passport Works Better Than Click-Through Training
Most practices now use some form of online training. It’s convenient, it prints certificates, and it looks tidy for CQC.
But here’s the problem: completion doesn’t equal understanding.
The tick-box trap
Online training often becomes a race to finish modules rather than a chance to learn. Staff click through the slides, take the quiz, download the certificate — and forget half of it by the next day. Managers see 100% completion and assume the team is compliant. In reality, few could explain how those policies apply in their daily work.
The Passport difference
The Professional Standards Passport turns that model upside-down.
It’s a pocket-sized handbook that brings together policies, standards, and personal development in one place. Staff keep it with them, use it in supervision, and record their reflections and progress.
It’s not just training — it’s learning in action.
- Staff take ownership of their own competence.
- Knowledge is available instantly on the job.
- Managers can see real evidence of reflection, not just a certificate.
- It supports “coffee-table” learning sessions and peer discussion.
Why it matters for CQC
The CQC’s Framework asks inspectors to find evidence that staff understand and apply the principles of safe, effective, caring, responsive, and well-led care.
The Passport provides that evidence directly — written by the people delivering the service.
The human factor
The Passport isn’t anti-technology. It’s pro-learning.
Where online systems measure attendance, the Passport measures absorption. It gives every staff member a reason to pause, think, and connect what they’ve read to what they do.
A better guarantee of real compliance
When training lives in a person’s pocket rather than on a computer, it becomes part of daily practice.
That’s the kind of lived compliance that survives inspections — and builds safer, stronger teams.
The Proof
The Winterbourne View incident showed that the Management had spent considerable resources to craft exemplary policies and system documents
However, this did not filter down to the frontline, usually becasue staff do not have the time or motivation to read and retain dozens of 20 page policies
A short focused policy is far more effective for learning, retention and application to real life
A Quick Comparison
| Subject | Digital LMS | Professional Standards Passport |
| Learning Model | Top-Down Delivery | Bottom-Up Reflection |
| Engagement | Passive | Active & Peer-Led |
| Evidence | Completion Certificates | Authored Reflections |
| Regulation 18 | Shows Training Given | Proves Competence Gained |
| Integrity | Tick-Box Risk | Personal Accountability |
| Cultural Effect | Compliance Fatigue | Reflective Practice |
Using our system as part of your defence in a CQC investigation
Case Study: False claims by disgruntled staff
Date: August 2025
Account by: Practice Manager
Location: Manchester
The CQC Complaint
Several disgruntled ex-employees got together to file “whistleblowing” complaint against the practice. The allegations included equity of access; failings in admin and governance; insufficient staff; stress at work; bullying and harassment; freedom to speak up …… and the kitchen sink !
We had no idea what evidence had been submitted to support the complaint.
- We had four days to respond.
- Failure to provide assurance would trigger a same-day unannounced visit.
How We Prepared
- Preparation extended well beyond documents.
- Reception and Admin staff focused on patient communication protocols, clinicians reviewed compliance logs, and managers checked evidence folders and were ready with an action plan.
- Clear communication ensured that everyone understood their responsibilities if inspectors arrived without notice.
How We Responded
- We acknowledged shortcomings where appropriate and presented clear action plans to address any gaps.
- We countered inaccurate claims with a robust defence supported by actual evidence.
- We showed our best in class “inspection-ready” system, incorporating a full annual compliance plan, and pointed the CQC to our suppliers web site
The Outcome
The CQC accepted our defence and were assured that we had a robust Quality Management System in place.
The case was closed and all action suspended.
What Saved the Day
The ability to compile a convincing defence in a professional manner is critical. Having dealt with inspectors over many years, the first port of call was to connect with the inspector to establish a working relationship. Familiarity with all types of systems from Ardens to TeamNet, and from Practice Index, QCS and FPM, made evidence gathering that much easier.
For Governance side, just 3 months ago we purchased a Quality Standards System that is fast becoming a National Standard. We explained this system to the CQC, and they checked out our supplier site.
With virtually no preparation, we were able to assure the Inspector that: -
- We had an ISO 9001:2015 “inspection-ready anytime” system, incorporating a full annual compliance plan
- It was a recognised Governance system to demonstrate HSCA and CQC Guidance compliance
- We had an “Interview-ready” staff handbook, including Appraisals, personal development; competency and knowledge; critical policies
- The system created a culture of self-responsibility and engagement where staff monitored their own competency; trained each other; and organised their own workshops
Key Takeaways: When dealing with a potential investigation
- Demonstrate you are Well-Led and well managed; show that this was just an anomaly
- Demonstrate that you have a robust Governance System; show how you operate in practice
- Prepare your systems early; It's too late to start when they knock on the door
Product used:
Quality Standards Manual: A structured approach to being inspection-ready anytime
Staff Passports: A personal Staff Development handbook for every member of staff, containing Appraisals, CPD record; Best Practice Knowledge; Key Policies. Creates a culture of self-responsibility and teamwork.
When it comes to compliance, many practices feel under pressure to keep updating their policy documents year after year. But the reality is very different: regulations hardly change.
The Truth About Policy "Updates"
Most so-called "updates" are minor tweaks—small changes to wording, layout, or grammar. Rarely do they involve substantive legal changes.
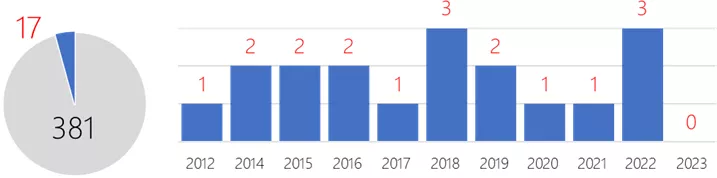
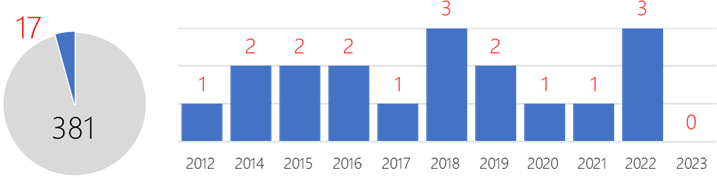
We analysed 10 years of legislation (2012–2023) and found:
- Out of 398 new laws, just 17 affected providers.
- That averages only 1 or 2 meaningful changes per year.
- In 2023, there were no relevant new laws at all.
Key Legislative Changes Since 2012
Here are the substantive changes that actually matter for providers:
| Legislation | Year | Relevance |
|---|---|---|
| Health and Care Act | 2022 | All Providers |
| Approved Premises (Substance Testing) Act | 2022 | Substance Abuse |
| Down Syndrome Act | 2022 | All Providers |
| Botulinum Toxin and Cosmetic Fillers (Children) Act | 2021 | All Providers |
| Coronavirus Act | 2020 | All Providers |
| Mental Capacity (Amendment) Act | 2019 | All Providers |
| Organ Donation (Deemed Consent) Act | 2019 | Hospitals |
| Health & Social Care (National Data Guardian) Act | 2018 | All Providers |
| Mental Health Units (Use of Force) Act | 2018 | Hospitals |
| Assaults on Emergency Workers Act | 2018 | Ambulance |
| Children and Social Work Act | 2017 | Adult Social Care |
| Immigration Act | 2016 | All Providers |
| NHS (Charitable Trusts Etc) Act | 2016 | Hospitals |
| Health Service Commissioner for England (Complaint Handling) Act | 2015 | All Providers |
| Health and Social Care (Safety and Quality) Act | 2015 | All Providers |
| Care Act | 2014 | All Providers |
| Immigration Act | 2014 | All Providers |
| Mental Health (Approval Functions) Act | 2012 | All Providers |
That's it. Fewer than 20 laws in a decade have made a real difference to provider compliance obligations.
What Suppliers Won't Tell You About Costs
The compliance market is big business. Providers are often sold more than they need. Here's what's typically on offer:
What's Available
- Downloadable packages – around £300 or less, promising 500+ policies, procedures, letters, and templates.
- Online systems – £1,000–£2,000 per year, offering over 1,000 pages of guidance, with features like staff activity logs.
The Hidden Costs
- Time to read every policy: Between one and three months of solid work (most never attempt it).
- Staff training/testing via online systems: Adds administrative load and ongoing management time.
- Briefing and testing staff knowledge: For a small organisation, this can equate to £15,000 in annual costs.
Saving Time and Money
Here's the bottom line:
- Suppliers have little incentive to tell you the truth. If they admitted you only need 50 core policies, and that legislation changes maybe once a year, their model collapses.
- You do not need a policy for every occasion. A well-written standard policy, applied with common sense, usually covers most scenarios.
- Use policy packages selectively. If you're buying a large library, treat it as a reference resource—not a manual that must all be implemented.
Key Takeaway
Regulations are relatively stable, and the real compliance burden is often overstated. Instead of drowning in hundreds of documents, invest in a concise set of core policies, keep an eye on genuine legal changes, and focus on training staff to apply good judgement.
In other words: compliance is about people, not paperwork.
Would you like me to combine this with the previous blog (on number of policies) into a longer guide-style article, or keep them as two separate, more focused posts?
This depends on the size of your organisation and the purpose of your policies.
This is what you should aim to have for a typical organisation with less that 50 staff:-
| CQC Policies | 20 to 30 |
| HR | 5 to 10 |
| Health & Safety | 5 to 10 |
| Admin | 5 to 10 |
For larger organisations, the numbers might go up by say 20% due to the complexities of dealing with stricter and more centralised systems.
Minimise the number of policies
- Focus on key policies and get them right
- A common sense approach to safety will cover most unusual situations
- It is better to invest time in developing staff and instilling common sense
- Do not overwhelm staff with paperwork to cover every eventuality.
CQC says they're not that interested
Is it about policies?
"Absolutely not. We are much less interested in policies and protocols than in knowing what care is like for your patients, whether staff know what to do about things like child protection, and so on. Good practices shouldn't need to do anything they aren't already doing."
Professor David Haslam, National Clinical Adviser to the Care Quality Commission
(Interview in Healthcare Leader News May 2012)
"We won't normally spend a great deal of time reading policy or procedure documents, unless we need to look at them to substantiate other evidence or what staff or patients have told us about their experiences."
James Hedges, media officer at the CQC (statement to MDDUS May 2013)
This is where the CQC focus their inspections:-
- Experiences people have when they receive care and the impact the care has on their health and well-being.
- Talking to patients, their families and their carers.
- Looking at records or speaking with staff and how they reach their judgements.
British Medical Association says don't bother with large numbers
Question: Is 'CQC' all about policies and protocols?
What the BMA says:
"We believe that most providers will already be compliant with the essential standards" and "CQC registration should not involve the development of large numbers of new policies and protocols."
Extracts from the BMA CQC Registration guidance for GPs.
|
How do you overturn a poor rating? When Providers get a poor rating, most will work hard to fix the issues, as no one wants the negatve publicity |
|
|
Summary of CQC Response
|
|
|
PLAIN ENGLISH SUMMARY OF THE CQC RESPONSE CONTEXT CQC RESPONSE CQC POLICY ON REINSPECTION CQC RISK BASED TARGETTING • CQC is focused mainly on finding new services at risk THE EFFECT ON PROVIDERS In effect, these Providers are trapped in a system where a negative rating becomes a permanent stain, almost impossible to remove. FUTURE PLANS Changes to the framework are underway, the CQC states “Work is therefore currently underway to improve how we use our new regulatory approach” |
|
| Link to the Freedom of Information Request | |
CQC Inspections Inspections dates have become corrupted
The “Publication date” was originally designed to represent a single type of event, being a site-inspection. This is now redundant as the Single Assessment Framework now adds several types of inspections and assessments ranging from a minor review to a full site inspection.
The Data Sheets are no longer fit for purpose as the “publication date” now creates a misleading impression as to the real status of inspection
This request is broken down into parts to enable you to provide clear and concise responses to each specific area.
FREEDOM OF INSPECTION REQUEST
For inspections carried out under the Single Assessment Framework, please provide updated data sheets that include information on each Quality Statement reviewed as follows:-
1. Date the Quality Statement was reviewed
2. Score achieved for that Quality Statement
3. Evidence quality: Whether via Site Inspection OR Remote/Other Review
CQC Response
Refused because: CQC estimates to search our records for the requested information would take significantly longer than 18 hours and we are therefore refusing to comply with any part of it.
Editors comments
This is a trivial exercise of exporting data from the main database, which the CQC do and publish every month
A SQL programmer could probably do this in 30 minutes
We believe the real reason is that it would be embarrasing for the CQC to admit that the ratings data has become corrupted as it mixes up two completely different Frameworks
In addition, it would also expose that on-site inspections have fallen to such an extent as to make them meaningless
Link: https://www.whatdotheyknow.com/request/single_assessment_framework_tran_2#incoming-2870031
Differentiate data between old KLOEs Vs New Single Assessment Framework
The “Publication date” was originally designed to represent a single type of event, being a site-inspection. This is now redundant as the Single Assessment Framework now adds several types of inspections and assessments ranging from a minor review to a full site inspection.
The Data Sheets are no longer fit for purpose as the “publication date” now creates a misleading impression as to the real status of inspection
This request is broken down into parts to enable you to provide clear and concise responses to each specific area.
FREEDOM OF INSPECTION REQUEST
Please provide updated data sheets which identify the following:-
Differentiation of inspections carried out under different systems:-
1. Inspections under the old KLOEs system
2. Inspections carried out under the new Single Assessment Framework
CQC Response
Refused because: CQC estimates to search our records for the requested information would take significantly longer than 18 hours and we are therefore refusing to comply with any part of it.
Editors comments
This is a trivial exercise of exporting data from the main database, which the CQC do and publish every month
A SQL programmer could probably do this in 30 minutes
We believe the real reason is that it would be embarrasing for the CQC to admit that the ratings data has become corrupted as it mixes up two completely different Frameworks
In addition, it would also expose that on-site inspections have fallen to such an extent as to make them meaningless
Link: https://www.whatdotheyknow.com/request/single_assessment_framework_tran#incoming-2870030
Misleading ratings on CQC site
During this transition to the new Single Assessment Framework (SAF), the public facing web site will show a range of “hybrid inspections” ranging from an old KLOE based inspections to partial application of the SAF to a full SAF based inspection. For the data to be meaningful and transparent, it is important that the Public have a clear and easily digestible picture of the level of checks and the exact dates these were carried out.
EXAMPLE TO ILLUSTRATE THE ISSUE:
In total, the SAF has 34 Quality Statements with 6 Evidence Categories each, giving a grand total of 204 potential measuring points for a full assessment or inspection.
From a recent live example on the CQC web site:
When a single Key Question “equity of access” is reviewed via a telephone interview, the remaining 203 evidence category are scored and updated to the latest SAF formulas based purely on the previous rating.
The date of the latest assessment is displayed at the top on the main page and on each Domain page to inform the Public about the age and reliability of this report and assessment.
THE ISSUE
The information displayed omits the critical facts that:-
1. only ONE Evidence Category out of 204 was checked
2. that the latest assessment represents 0.5% of the potential items that could be checked
3. that 99.5% of the updated items are from a real site-inspection
4. that the evidence for the 99.5% updated items is in actuality 5 years out of date.
FREEDOM OF INFORMATION REQUEST
Please provide details of what steps the CQC has taken to address this anomaly so that the public is assured of transparent and easily understood information regarding:-
1. the number of Evidence Categories that were reviewed
2. the date/age of each review
3. differentiating evidence obtained at actual site-inspections
CQC Response
In accordance with section 1(1) of FOIA we are able to confirm that CQC does hold recorded information in relation to this matter.
CQC does not display scoring information down to the evidence category level on our website.
We are currently working on finalising the automation of our publication and will then be delivering design improvements to our reports on the website. This improvement work is currently scheduled to start at the end of October.
Editor's comments
CQC did not address the issue and did not suply the information awaiting improvements in October 2024
Following this request, the CQC scrapped the Evidence Ratings altogether
Link: https://www.whatdotheyknow.com/request/single_assessment_framework_prov#outgoing-1734540
CQC
Formal CQC process for managing requests for a re-inspection
We have recently received the following response from a member of your team with reference to improving ratings following an inspection:-
“…… providers generally cannot request a re-inspection. If a provider did ask us to re-inspect their service, we would likely consider their request and any specific factors around this, but there is no formal process for this as we generally focus our resources on services where there is risk.”
As at June 2024, there appear to be some 9,158 providers with some level of poor rating, with 7,876 dating back to between 2019 and 2023 and 642 dated 2018 or older, who are effectively barred from improving their rating even for relatively minor infractions where documentary evidence of improvement could be sufficient, without requiring a site visit.
It is of concern that there is no formal process to manage a provider request for reinspection.
Furthermore there is a contradiction in policy where resources are allocated to “where there is risk” but inexplicably excludes thousands of providers already identified as high risk.
FOI REQUEST: MANAGING REQUESTS FOR RE-INSPECTION:-
1. If the process exists, please provide details together with reasons why this is not published on the CQC web site
2. If the process does not exist, please provide details of when and how this will be rectified
CQC Response
There is no formal process for providers to request an assessment to change their rating, nor are there plans to introduce such a process.
Editor's Comment
Regardless of the improvements made, there is no pathway to remove the stigma of a negative rating, which must be displayed prominently on web sites, and can remain unchanged for up to 10 years.
At the date of this request, there are almost 8,000 Providers stuck with negative ratings which are up to 5 years out of date.
In effect, these Providers are trapped in a system where a negative rating becomes a permanent stain, almost impossible to remove.
Link: https://www.whatdotheyknow.com/request/formal_cqc_process_for_managing#outgoing-1734527
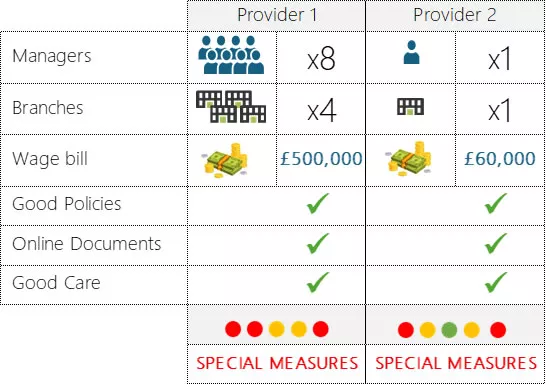
How these providers failed at everything all at once
We looked at two particular inspection failures, one had as many resources as you could wish for and another being your usual smaller provider with one Manager.
Both had comprehensive policies; an online document management system; and generally provided good care.
Things ran smoothly. Everything looked fine.
At The inspection
It all looked good on paper, so the CQC Rating came as a shocker.
Senior Management is shocked!
Information isn’t to hand, processes are not always followed, there are gaps in the system, things are not done properly.
2024 Inspections will be even more challenging as the focus shifts to “Feedback” which most systems are not designed for
This rating will stay on their web site until the next inspection. That could be the next 5 Years, unless you ask for a reinspection.
Lessons learnt
- It is not just about having the best policies or more human resources
- 99% of the inspection is about continuous compliance
- Don’t let the inspector be the first to find your weaknesses
The solution
CQC inspections are based on your performance over the last 12-24 months. By the time an inspection is announced, it is already too late to prepare.
The registered Manager is central to an inspection. The uncomfortable truth is that the Registered Manager delegated everything, did not monitor, and took their eye off the ball.
You must be inspection-ready anytime, and your system should tell you this at the press of a button.
Apps for a robust Clinical Audits System.
A Clinical Audit System should comprise two elements:-
- An effective Policy and Governance
- A consistent process that records each audit
Our system will enable you to achieve these with two applications in tandem:-
- Risk Assessment Channel
A comprehensive Risk Assessment based on the guide by NICE; CHI,RCN, University of Leicester.
This is a living document that combines Risk Assessment, Governance, and Policy Statement in one. The initial “one-off” review should take no more than 10 minutes to complete, and the Dashboard will automatically generate a Risk Matrix together with a risk rated Governance and Policy Document, incorporating National Best Practice as published by NICE.
Regular reviews should take no more than 5 minutes at most, best be done as a team exercise as part of the individual clinical audits. This automatically achieves group training and development; enables discussion of improvement strategies; and acts as a team refresher and briefing, to demonstrate leadership and Well-Led criterion.
- Processes Channel: Clinical Audits Record
The process for conducting regular Clinical Audits is to be found in the “Quality Audits” section in the Processes Channel.
This App covers the required principles of Topic Selection; Criteria; Standards; Outcomes; and Reflection, ensuring your approach meets the stringent NICE standards. A printable checklist allows offline planning, training and general discussion of the principles before the formal meeting.
Recording the process and outcomes takes just minutes, and the Dashboard will automatically generate your log of audits with a detailed record of your risk rated decision making.
Benefits:-
The ready-made processes take no more than a few minutes to record, and ensure that we follow a stringent quality process mapped directly to the highest standards.
What you will achieve is:-
- A record of adherence to National Standards
- Consistent and structured approach to every Clinical Audit
- Dashboards to show Risk Analytics
CQC needs clinical oversight by a member of the team for has a good working knowledge of medical and nursing domains, QoF and audits etc.
When the call comes from CQC that individual is then placed to have a good understanding of where their organisation is…
I recently had an e-mail from CQC inspector who had received an anonymous complaint about our service. This covered four key aspects of our organisation: complaints, staff appraisals, infection control and fire risk assessment.
Having used package from everything CQC I was able to quickly place my hands on the key audits and information the inspector required, going back to her within 16 hours, with a positive outcome “Thank you so much for your quick, comprehensive and clear responses”.
It isn't enough to hand the responsibility to a practice manage or deputy, as the registered manager you need a good system to support you in the role.
Dr Benjamin Kay
Harcourt Medical Centre
IPC Risk Assessed in ONE Day
98% NHS England audit score
1. The Challenge:
I joined as the interim PM of this Practice and one of my first urgent tasks was to complete the IPC audit for an imminent NHS England IPC Audit.
This was a bigger challenge than I had anticipated as there was nothing to work from, the last IPC Risk Assessment was done some 4 years ago and could not be located. There were limited regular checks, and as with many smaller Practices, there were limited staff and resources.
The Lead Nurse was faced with the daunting prospect of the 45-page NHS IPC Audit, which would have taken 3 to 6 weeks to implement on her own, with no other resource that would allow her to meet the robust requirements in such a short space of time and the inspection was due in 2 weeks.
The challenge was two-fold: Doing an IPC Risk Assessment to National Standards in a short time frame, identifying and fixing any potential issues before the auditors arrived. The only viable option seemed to be contracting an independent commercial audit.
2. NHSE Audits:
NHSE inspectors take a constructive approach in getting practices compliant.
However, a low score will likely trigger a CQC inspection as the IPC team is duty-bound to notify the CQC.
3. Solution:
By happenstance, we found that X-Genics, our Compliance System provider, was testing a prototype IPC Audit tool based directly on the NHS Toolkit and international best practice and were looking for volunteers to field test it before launch. This system was part of the digital automation bid project, we had collaborated on and had already implemented this bespoke automation software solution for general CQC Compliance and IIF Reporting.
4. How we did it
The process turned out to be both simpler and faster than we had expected.
How the system works:-
- The National Standards are broken down into bite sized mini-Apps.
- Each App has an integrated mini checklist(s) to easily manage individual IPC areas.
- Each checklist is delegated to different staff, spreading the workload across the practice.
- Results are collated, risk evaluated and summarised into the App.
- Automatic Dashboards generate an Action Planner and Risk Matrix
- Action Points are addressed, and the Apps updated.
- Checklists are reused daily/weekly/monthly to achieve continuous compliance.
- The process of evaluation and summarising into the App is repeated through the year.
We distributed the user-friendly checklists to our staff, outlining specific tasks for hazard review. Each staff member received a checklist, and they were tasked with assessing and reporting on identified hazards, and staff were encouraged to fix minor issues on the spot. The nursing team and practice manager took charge of conducting reviews in key and high-risk areas. We added an element of fun by offering chocolates as rewards for timely completion and team achievements.
After completing the assessments, the checklists were collected the following day, and entered into the mini-apps. The software generated a user-friendly visual plan, with our risk mitigation steps, and our action plan for any outstanding action points.
Our strategy focused on starting with low-risk items that were more easily manageable and within our immediate control. Having achieved these "easy wins" and gaining experience, we progressed to focusing resources on higher risk areas. Identifying at an early stage, areas that required external assistance. For instance, we identified that the original door handles in a converted residential property were not easily wipeable, necessitating replacement and scheduled this in as an action point.
5. Completion:
This approach created an efficient workflow and allowed us to tackle potential risks in a systematic manner, prioritising actions to achieve maximum impact with minimum effort.
There was zero training needed. The entire IPC Risk Assessment was completed in one day, leaving sufficient time to address issues for remedial action.
6. Outcome:
98% score achieved at the NHS England audit two weeks after our risk assessment.
We achieved well over 100% return on investment compared to external contractors, on this App alone, and have started using others such as Fire Risk Assessment. We have taken full control of IPC, and this has now become continuous compliance instead of an annual exercise.
Going forward, the checklists are now used as our regular reviews, and results used to update the Apps. In addition, we rotate the staff and checklists, so staff learn about a different area every month, in effect a continuous training regime by “learning on the job”.
All staff feel empowered, engaged and enthused with their new responsibilities, a total culture change for the Practice, and a reduced workload for the Manager and Lead Nurse. In effect, our IPC runs automatically and autonomously thanks to our motivated staff.
7. Improvements:
- We are IPC inspection ready at all times
- Professional compliance reports at the press of a button
- Saved the cost of external contractors
- Continuous Risk Assessments carried out every month at no extra cost
- A positive IPC Culture
- Reduced management workload
- Formal training sessions largely replaced by training on the job
- Staff teach each other when uncertain
8. Credits:
Author: Shabana Dehlavi Provider type: GP Practice Date of study: February 2024
The system supplier is X-Genics via their CQC focused web site everythingCQC.com.
The Audit and Risk Assessment Channel includes risk assessments for Infection Control and Fire Risk; with COSHH, Display and Screen Equipment and Safeguarding currently in the pipeline.
Case Study:
Investment and Impact Fund – NHS England
Turning a Simple Spreadsheet into a £20,000 Income in One Week
Introduction
IIF, or Investment and Impact Fund, is a funding mechanism in the UK that provides financial incentives to general practices for improving their performance in various areas, such as immunizations, cancer screening, and chronic disease management. However, tracking and reporting on the progress and achievements of these targets can be a tedious and time-consuming task for practices, especially when working collaboratively in a Primary Care Network (PCN). This case study outlines how a group of practices in a PCN used a simple spreadsheet and a mini-app platform to develop an innovative solution that not only made tracking and reporting more efficient but also helped them identify missed opportunities and easy wins, resulting in a £20,000 income in one week.
The Problem
The practices in the PCN were struggling to keep up with the IIF targets due to various reasons, including the complexity of the funding mechanism, lack of clarity on what to do next after identifying gaps, and the burden of communicating and reporting the progress to PCN managers. This is the first year practices have had a high amount of incentivised indicators to achieve, with the potential for missed opportunities and underperformance. To address these challenges, the practices decided to develop a simple yet effective solution that would not only make tracking and reporting more efficient but also help them engage and motivate each other.
The Design
The practices used a mini-app platform called eManager by X-Genics to create a custom solution that would allow them to enter data quickly and generate automated dashboards that provided instant insights into missed opportunities and easy wins. The solution was designed to focus on forward planning rather than looking back, with a month-by-month record of achievements and missed targets. The solution was financially focused, highlighting the value of missed targets and identifying easy-to-reach targets. It automatically highlighted priorities and made it easy to understand and plan. Importantly, the solution was designed to engage practices by making every practice enter data and self-examine, resulting in better targeting of patients, focused meetings on group-wide achievements, and better collaboration across the network.
Achievements
The solution had a significant impact on the practices and the PCN, resulting in a £20,000 income in one week. The financially focused dashboard enabled the practices to differentiate profitable indicators from easy kills, resulting in better decision-making and a more targeted approach to achieving the IIF targets. The practices reported better engagement and collaboration, with all four practices working together in this and other areas, resulting in a joint Patient Participation Group (PPG) for better use of common resources. The solution enabled the practices to track progression over 12 months, plan and achieve goals without any last-minute rush, and identify coding errors. The practices reported that they achieved £20,000 across the PCN in the first two weeks of using the solution, and they understood how to work with IIF for the first time as a team.
Using a fully managed system and automated Dashboards, has allowed the team to focus on performance, never having to worry about updates to the requirements or the latest version of spreadsheets. The impact on the team is evident in a single comment by Dr Peter Brown the Clinical Director of Northwest Merton PCN said “I don’t know how other PCN’s are managing without this”.
Practice Managers reported feeling a sense of achievement and feeling valued as they were able to make more effective contributions to financial performance and clinical quality measures.
“So far the system has made a real impact on visualising targets and added value as well as holding practices accountable for their end of delivery.” Said Pinar Johnson, PCN Manager of Northwest Merton PCN
Conclusion
The IIF case study demonstrates how a simple app platform that generates intelligent Dashboards can be used to develop innovative solutions to address complex teamwork challenges in the healthcare system. The practices in the PCN were able to turn a tedious and time-consuming task into a financially profitable one, using a focused dashboard that not only made tracking and reporting more efficient but also helped them identify missed opportunities and easy wins, resulting in a £20,000 income in one week. The solution enabled the practices to engage and motivate each other, resulting in better collaboration and decision-making. The success of the solution can be attributed to the practices' focus on planning forward, financially focused design, and engagement of every practice in the network.
The system can be used solely by the PCN Manager to input already consolidated data, but involving and engaging member practices has the added benefits of self-responsibility; effective delegation; grass root improvements; and individual learning, not to mention that it makes the PCN Managers life that much easier.
Single Assessment Framework: Quality Statements and Key Lines Vs Enquiry (KLOEs)
Is there a transition period from KLOEs to Single Assessment Framework
Background:
In 2022 the CQC announced providers will start to be regulated against the new single assessment framework from January 2023, and that the Quality Statements in this framework replace the previous Key Lines of Enquiry (KLOEs).
On 21 December 2022, the CQC announced a revised plan stating that the new assessment framework will begin towards the end of 2023.
The issue:
Evidence for an inspection or assessment by nature constitutes past performance, meaning that at the time of the inspection in say January 2024, the provider would need to demonstrate they were in compliance with the new Quality Standards for a pre-defined period prior to that date.
The whole of 2023 now becomes a transition gap between KLOEs phased out and a new framework coming into play, and providers need clarification as to which system to follow; when to stop the old Vs the new; and what they will be judged on at the beginning of the new regime.
The request: Please clarify:
1. The status of the KLOEs between now and the end of 2023, specifically their applicability and actual usage by inspection teams in this period.
2. The status of the Quality Statements between now and the end of 2023, specifically whether providers should prepare compliance based on these from this point forward OR only from the end of 2023 OR use both these and KLOEs in parallel.
It is important that your response is definitive as providers will rely on this and expend considerable resources over the next 12 months to be prepared for the new assessment framework.
Yours faithfully,
Editor everythingCQC
CQC Response
We have committed to being clear when the framework will directly affect health and care providers (see link below) and will give clear notice of the date from which assessments using the Single Assessment Framework will be made. Until that notice is given, we will continue our current methods to monitor, assess and rate providers. We will continue to provide updates as to the scope and status of our current inspection programme.
Editor's comments
In summary: CQC made no transitional arrangement. Providers have to use the old system until the day the SAF comes into force
Therefore, on day one CQC Inspectors will start inspecting on the new Framework, but every provider will have been using the old Framework
As a result of this this enquiry, the CQC postponed the entire Single Assessment Framework to November 2023
Link: https://www.whatdotheyknow.com/request/single_assessment_framework_qual#outgoing-1417089
| Project for a unique automation solution for Practice Management | |
| Project initiated by: | South West London Digital First (SWL CCG) |
| Commissioned by: | Group of SW London PCNs |
| Project led by: | Northwest Merton Primary Care Network |
| Initial Pilots enrolled in programme: |
|
| Status: | Initial pilots have been completed and commercial roll out commences November 2022 |
| Funding: | Qualifies for PCN Development Budget |
| Objectives | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This will also make it possible to achieve and be certified to a recognised level such as the International ISO 9001:2015 standard with less effort, and act as a benchmark of assurance to minimise the burden for CQC Inspectors. This project will address the following: -
Peer Support Network A common standard and common practices are essential building blocks for collaboration and efficiencies at scale. Digitisation will provide risk measured performance data, which can be used to pinpoint weaknesses to effect improvement. Based on a centralised and real-time record of activity, we intend to introduce new ways of support and collaboration at PCN level. This will include: -
PCN Level Management:
Quality Assurance & CQC Inspections:
Engagement with ICSs and Local Authorities: The proposed system has the capability of “Channels” for other Stakeholders, which can be workflow Apps or simple data collection instruments, Examples of usage are:-
Business Continuity Risk:
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The key benefits of this system are: -
Benefit for PCNs PCNs will achieve instant economies of scale with zero effort. Their library of common Best Practices is maintained centrally with automatic updates. Setup takes minutes, and the system is simple and intuitive, taking a couple of minutes to learn.
Automation will free up Practice Managers, the most valuable member of the team, for more productive tasks. Standardisation of Best Practice and streamlining of processes will provide consistency of service quality. Patients can be assured that their Provider is adhering to a high-quality standard on a continuous basis and not just at a single point in time of the CQC Inspection. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
(100 words max scored)
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The first batch of Trial Versions will be sent out from early November. Initial Expressions of Interest indicate high demand. Priority will be given to PCNs and subject to slots available on the waiting list. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||













